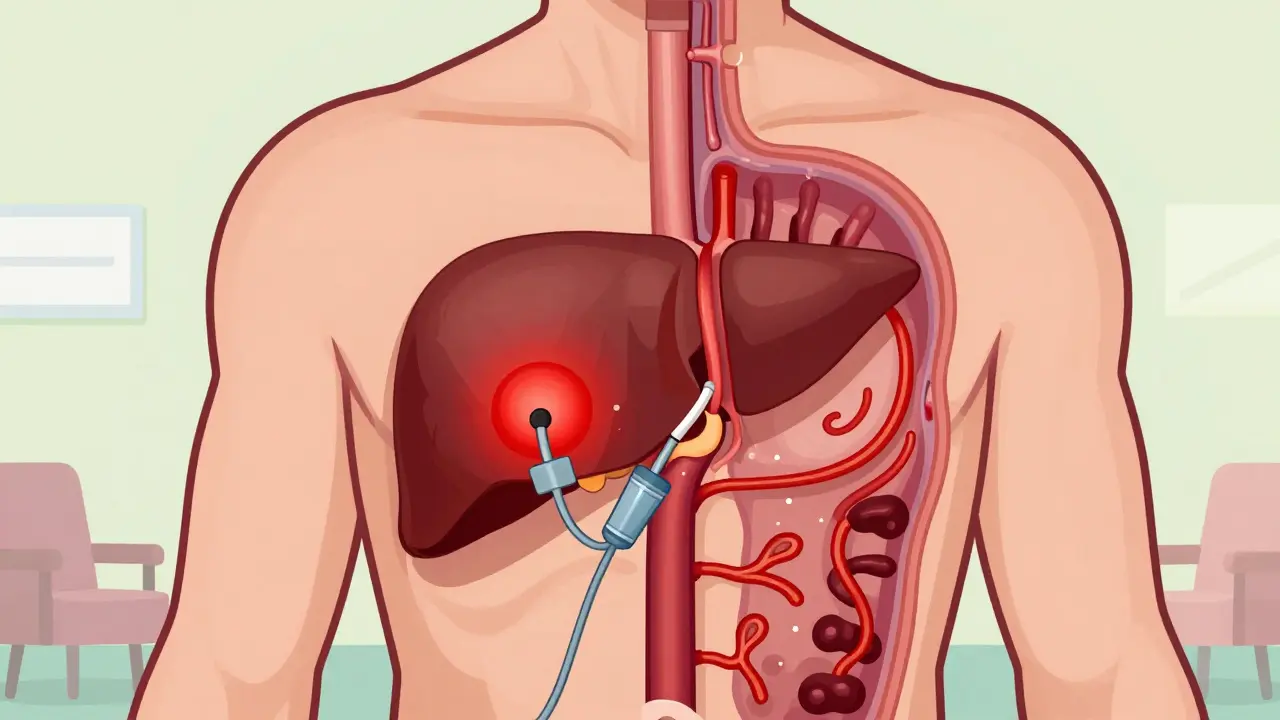
When your liver is damaged by cirrhosis, pressure builds up in the portal vein-the main blood vessel that carries blood from your intestines to your liver. This pressure forces blood to find new pathways, creating swollen, fragile veins in your esophagus or stomach. These are called varices. And when they rupture? It’s a medical emergency. About 1 in 5 people with variceal bleeding die within six weeks. That’s why knowing how to stop it, prevent it, and manage it isn’t just important-it’s life-saving.
What Happens During a Variceal Bleed?
Variceal bleeding doesn’t start with pain. It starts with internal pressure. In cirrhosis, scar tissue blocks blood flow through the liver. Blood backs up, and veins in the esophagus or upper stomach stretch like overfilled balloons. They’re thin-walled, not meant to handle high pressure. A sudden spike-like from coughing, vomiting, or even straining-can cause them to burst. The result? Vomiting bright red blood or passing dark, tarry stools. Many patients collapse before they even make it to the hospital.
Doctors don’t wait. Time is everything. The first 12 hours after bleeding starts are the most critical. That’s why guidelines from the American Association for the Study of Liver Diseases (AASLD) say endoscopic band ligation must be done within this window. Delay it, and your chances of survival drop.
Endoscopic Band Ligation: The Gold Standard
Endoscopic band ligation (EBL) is now the go-to treatment for stopping active bleeding. It’s simple in concept: a tiny rubber band is placed around the swollen vein, cutting off its blood supply. The vein shrinks, clots, and eventually disappears. Modern devices like the Boston Scientific Six-Shot Banding System can place up to eight bands in one session, cutting procedure time by 35% compared to older single-band tools.
Success rates are high-90% to 95% of patients stop bleeding after one session. But one session isn’t enough. Varices don’t vanish overnight. Most people need three to four treatments, spaced one to two weeks apart, to fully eliminate them. Each session costs between $1,200 and $1,800 in the U.S., and while it’s effective, it’s not easy. Some patients report severe throat pain for weeks after the procedure, making swallowing painful. Others describe it as a relief: "Band ligation stopped my bleeding immediately. I was out of the hospital in three days."
Still, it’s not perfect. In cases of heavy, active bleeding, the endoscope can’t always see clearly. Failure rates climb to 10-15% in these situations. That’s why banding is never used alone. It’s always paired with medication.
Beta-Blockers: The Silent Shields
While banding stops the bleeding, beta-blockers prevent it from happening again. Non-selective beta-blockers (NSBBs) like propranolol and carvedilol work by slowing your heart rate and reducing blood flow to the liver. This lowers the pressure in the portal vein by 15% to 25%. The goal? Bring the hepatic venous pressure gradient (HVPG) down to 12 mmHg or lower-or at least cut it by 20% from baseline.
Carvedilol has become a favorite. A 2021 study in Hepatology showed it lowers portal pressure better than propranolol (22% vs. 15%). Both cut rebleeding risk by about half compared to no treatment. But here’s the catch: not everyone can take them. Side effects like fatigue, dizziness, and low blood pressure make them hard to tolerate. About one in four patients can’t reach the full dose. One Reddit user wrote: "Propranolol made me so tired I couldn’t get out of bed. I switched to carvedilol-it works better, but costs $35 a month."
Propranolol is cheap-$4 to $10 a month as a generic. Carvedilol? $25 to $40. Insurance doesn’t always cover the difference. For patients on tight budgets, this isn’t just a medical choice-it’s a financial one.

Why You Can’t Rely on Beta-Blockers Alone
Even though beta-blockers prevent rebleeding, they don’t stop active bleeding. That’s a key point. The Baveno VII consensus in 2022 made it clear: using beta-blockers alone during an acute bleed only works about half the time. Banding, combined with medication, hits 90% success. That’s why guidelines now say: banding first, then beta-blockers.
And it’s not just about stopping the current bleed. For people who’ve never bled but have high-risk varices, NSBBs are used for prevention. Carvedilol is now being studied as a potential replacement for banding in this group. A 2023 study in the New England Journal of Medicine found carvedilol alone was just as effective as banding at preventing first-time bleeding. That could change how we treat people before they ever bleed.
When Banding and Beta-Blockers Aren’t Enough
Some patients don’t respond. Some rebleed. For them, there are other tools.
Transjugular intrahepatic portosystemic shunt (TIPS) is a procedure where a metal tube is placed between the portal vein and a liver vein, creating a pressure-release valve. It works well-1-year survival jumps from 61% to 86% in high-risk patients. But it comes with a big cost: 30% of people develop hepatic encephalopathy, a brain disorder caused by liver failure. It’s not for everyone.
For gastric varices (bleeding in the stomach), banding often fails. Doctors turn to balloon-occluded retrograde transvenous obliteration (BRTO). A 2023 analysis of over 7,000 patients showed BRTO cut 30-day mortality in half compared to banding alone. But BRTO isn’t widely available. Only 45% of U.S. hospitals have the interventional radiology teams needed to do it.
Vasoactive drugs like terlipressin and octreotide are used to buy time. Terlipressin cuts mortality by 34% in trials. Octreotide works just as well in real-world settings. Now, a new long-acting version of octreotide (Sandostatin LAR) lets patients get one injection a month instead of daily doses. Adherence has been a problem-only 62% of patients stick with daily shots. This could change that.
What’s Next?
The future of variceal bleeding management is getting smarter. The PORTAS trial is testing a new way to place TIPS through the spleen instead of the liver-making it easier to do in smaller hospitals. By 2027, that could bring TIPS to 75% of U.S. hospitals instead of the current 45%.
Artificial intelligence is also on the horizon. Researchers are training algorithms to predict who’s about to bleed by analyzing scans, lab values, and even voice patterns. Dr. Patrick Northup predicts AI could cut mortality by 40% in the next decade.
But the biggest barrier isn’t technology-it’s access. Uninsured patients are 35% more likely to die from variceal bleeding than those with insurance. Rural areas lack specialists. Emergency rooms often can’t get endoscopy done in time. Only 68% of hospitals meet the 12-hour window. And only 55% of patients reach the full beta-blocker dose within three months.
What You Need to Know
- If you have cirrhosis, get screened for varices-even if you feel fine.
- If you’ve bled, banding + beta-blockers are your best shot at survival.
- Carvedilol may be better than propranolol, but cost and side effects matter.
- TIPS saves lives but can cause brain fog. It’s for high-risk cases only.
- Don’t skip your banding sessions. Skipping one increases rebleeding risk by 50%.
- Use patient support programs. The American Liver Foundation offers nurse navigators to help with meds, appointments, and costs.
Variceal bleeding is scary. But it’s manageable. With the right combo of banding, medication, and follow-up, many people live for years. The key? Acting fast, staying consistent, and never giving up on the plan-even when it’s hard.



tatiana verdesoto
3 March 2026 - 19:02 PM
Just read this whole thing and I’m sitting here with tears in my eyes. My mom went through this last year. She didn’t even know she had cirrhosis until she started vomiting blood. Banding saved her life, but the side effects? Oof. She couldn’t eat solid food for weeks. I’m so glad someone wrote this clearly. No jargon, just truth.
Also, the part about carvedilol vs propranolol? My insurance denied it at first. Took three appeals and a letter from her hepatologist. If you’re struggling with meds, call the American Liver Foundation. They hooked us up with a free 30-day supply. Seriously. Do it.
And yes-skip a banding session? Bad idea. We missed one. She rebled. Two weeks in the ICU. Don’t let that be you.
Love you, liver warriors.
Jessica Chaloux
4 March 2026 - 09:44 AM
😭 I’ve been on propranolol for 3 years. My hands shake so bad I can’t hold a coffee cup. Carvedilol? Worth every penny. But yeah… $35 a month when you’re on SSDI? Not happening. 😔
Mariah Carle
4 March 2026 - 12:30 PM
There’s a metaphysical layer here, isn’t there? The liver as the silent guardian-overburdened, ignored, then violently betrayed by its own function. We treat varices like a mechanical failure, but what if it’s a soul-level cry? A body screaming, ‘I’ve held too much.’
Band ligation? A temporary fix. Beta-blockers? A chemical pacifier.
The real cure is stillness. Rest. Letting go of the pressure-emotional, financial, societal. Maybe that’s why some patients heal better when they stop fighting and start surrendering.
Just a thought. 🌿
RacRac Rachel
5 March 2026 - 03:44 AM
This is one of the most important posts I’ve read this year. Thank you for writing it with such clarity and heart.
For anyone reading this who has cirrhosis or knows someone who does: please, please, please get screened. Even if you feel fine. Varices don’t announce themselves. They don’t knock. They just… rupture.
I’m a nurse in rural Idaho. We lost three patients last month because their local ER couldn’t get an endoscopy done in time. The 12-hour window? It’s real. And it’s slipping away in places like mine.
If you can, advocate. Push. Call your rep. Demand better access. This isn’t just medicine-it’s justice.
You’re not alone. I see you. 💪❤️
Jane Ryan Ryder
6 March 2026 - 21:29 PM
Oh great. Another post telling me I’m dying because I drank too much. Newsflash: I didn’t choose cirrhosis. My dad did. His liver failed. Mine followed. And now I’m being told to pay $35/month for a drug that makes me feel like a zombie?
Meanwhile, my cousin’s cousin’s dog got a $12,000 surgery for a torn ACL. But me? I get told to ‘stay consistent.’
Thanks for the guilt trip, internet.
Callum Duffy
7 March 2026 - 10:17 AM
A most informative and meticulously structured exposition. The clinical precision with which the therapeutic modalities are delineated is commendable. One might reasonably infer that the integration of endoscopic intervention with pharmacological prophylaxis constitutes the current apex of evidence-based management.
That said, the socioeconomic disparities in access to care remain profoundly troubling. The 35% mortality differential between insured and uninsured patients is not merely a statistic-it is a systemic failure of moral imagination.
One hopes for policy reform before the next decade's data is compiled.
Levi Viloria
8 March 2026 - 10:48 AM
I’m from a small town in Mississippi. We don’t have a single hepatologist within 120 miles. Our ER docs do their best, but when the patient comes in vomiting blood and the nearest endoscopy unit is two hours away? It’s too late.
I’ve seen it too many times.
That’s why I started a nonprofit last year-Mobile Liver Care. We drive a van with portable ultrasound and a nurse practitioner to rural clinics. We screen, we educate, we connect people to meds.
It’s not TIPS. It’s not banding. But it’s something.
If you’re in a rural area and want help, DM me. We’ll find a way.
Richard Elric5111
8 March 2026 - 12:22 PM
One cannot help but observe the ontological paradox inherent in the management of variceal hemorrhage: we intervene mechanically to arrest a symptom while pharmacologically modulating a physiological response, yet we neglect the fundamental etiology-the cirrhotic liver itself.
Is it not a form of epistemological arrogance to believe that banding and beta-blockers constitute a cure, when in fact they are merely palliative accommodations to an irreversible structural collapse?
Perhaps the true therapeutic frontier lies not in the endoscope or the pharmacy, but in regenerative hepatology-the reconstitution of the organ, not the containment of its consequences.
Dean Jones
8 March 2026 - 15:04 PM
Let’s get real here. Everyone’s talking about banding and beta-blockers like they’re magic bullets. But here’s what no one’s saying out loud: most of these patients are already on their third or fourth liver failure. They’re 65, they’ve been drinking since they were 18, they’re on SSDI, they don’t have a family, and their only ‘support system’ is a Reddit post from a stranger.
Band ligation? Sure. Works great. If you can get to the hospital in 10 minutes. If you have a ride. If you’re not too dizzy from the propranolol to hold your keys. If your insurance hasn’t denied it because you ‘didn’t try the cheaper option first.’
And don’t even get me started on carvedilol vs propranolol. One’s a luxury item. The other’s a Walmart special. But the outcome? Same. You’re still dying. Just slower.
We’re treating symptoms like they’re choices. They’re not. They’re consequences. And we’re too damn scared to admit that.
So yeah. Banding works. Beta-blockers help. But if you’re poor, rural, or black? Your odds are still 3x worse. And no amount of clinical data changes that.
Fix the system. Not just the veins.
Zacharia Reda
10 March 2026 - 09:38 AM
Wait-so you’re telling me a $10 generic pill can cut rebleeding risk in half… but I can’t afford the $35 one that works better?
And the new long-acting octreotide? One shot a month? That’s genius. But only if you have a doctor who’ll prescribe it and a pharmacy that stocks it and a bus that gets you there.
Meanwhile, I’m over here Googling ‘how to stop bleeding at home’ because my last endoscopy was 11 months ago and I can’t afford the copay.
So yeah. Science is cool. But real life? It’s a mess.
Jeff Card
11 March 2026 - 17:14 PM
I lost my brother to this. He was 42. He didn’t drink. He had hepatitis C, got treated, thought he was fine. Didn’t get screened. One day, he just… didn’t wake up.
They found the bleed too late. No banding. No meds. Just a body.
If you have cirrhosis-even if you think you’re ‘cured’-get the scan. Even if you feel fine. Even if you’re scared. Even if you think it’s too late.
It’s not.
Sharon Lammas
12 March 2026 - 08:53 AM
Reading this made me think of my grandmother. She had cirrhosis from alcohol, but she never drank again after her diagnosis. She took her pills. She went to every banding session. She didn’t complain.
She lived 11 more years.
She didn’t do it because she was brave. She did it because she loved her grandkids too much to leave us.
That’s the real story behind every statistic.
Don’t forget that.
marjorie arsenault
13 March 2026 - 15:36 PM
You got this. Seriously. One banding session at a time. One pill at a time. You’re not alone. I’ve been there. I’m still here. And you can be too.
Call the ALF. They’ll help. I did. You can too. 💖
Deborah Dennis
14 March 2026 - 08:08 AM
Wow. So many words. And yet… no one’s saying the obvious: if you’re gonna have cirrhosis, why not just accept it? Why fight? Why spend thousands? Why go through banding? Why take pills that make you tired? Why not just… live your last days peacefully?
Maybe you’re not supposed to survive.
Just saying.