Primary Sclerosing Cholangitis, or PSC, isn’t a condition you hear about often-but for those living with it, it’s everything. It’s a rare, progressive disease that slowly destroys the bile ducts inside and outside the liver. When these ducts get scarred and narrowed, bile can’t flow the way it should. That’s when things start to go wrong: toxins build up, the liver gets damaged, and over time, cirrhosis and liver failure can follow. There’s no cure. No magic pill. And for many, the road to diagnosis is long, frustrating, and lonely.
What Exactly Happens in Your Body With PSC?
PSC attacks the bile ducts-tubes that carry bile from the liver to the intestines. In healthy people, these ducts are smooth and wide, around 3 to 8 millimeters across. In PSC, inflammation turns them into stiff, scarred tunnels, sometimes shrinking to under 1.5 mm. This isn’t just a minor blockage. It’s a slow, silent choking of the liver’s natural detox system.
The damage doesn’t happen overnight. It follows four clear stages:
- Stage 1: Inflammation starts in the portal areas of the liver.
- Stage 2: Fibrosis begins to spread around the portal zones.
- Stage 3: Bridges of scar tissue form between liver areas, disrupting blood flow.
- Stage 4: Cirrhosis sets in-the liver becomes a patchwork of scar and dead tissue.
Most people are diagnosed between ages 30 and 50, with men being twice as likely to develop it as women. The disease progresses differently for everyone. Some stay stable for years. Others see rapid decline. On average, it takes 12 to 15 years from the first symptoms to full cirrhosis.
Why Do People Get PSC? The Gut-Liver Connection
Doctors still don’t know exactly what triggers PSC. But one thing is clear: it’s not just the liver. It’s the gut too.
Up to 80% of people with PSC also have inflammatory bowel disease-most often ulcerative colitis. That’s not a coincidence. Research now shows the gut and liver are deeply linked. When the gut lining becomes leaky or the microbiome goes out of balance, certain bacterial byproducts travel through the bloodstream and trigger an immune attack on the bile ducts.
Genetics play a role too. People with the HLA-B*08:01 gene variant are over twice as likely to develop PSC. But genes alone don’t cause it. Something in the environment-maybe an infection, a diet, or an immune trigger-turns on the disease in those who are genetically at risk.
Unlike Primary Biliary Cholangitis (PBC), which targets tiny bile ducts and shows clear antibody markers, PSC is sneakier. Only half of patients test positive for p-ANCA, and there’s no single blood test that confirms it. Diagnosis relies on imaging-usually MRCP (magnetic resonance cholangiopancreatography)-to see the characteristic beaded pattern of narrowed ducts.
Symptoms Are Subtle… Until They’re Not
Many people with PSC feel fine for years. That’s why it’s often found by accident during routine blood tests showing high liver enzymes-especially ALP (alkaline phosphatase).
When symptoms do appear, they’re frustratingly vague:
- Fatigue: 92% of patients report this. Not just "tired"-bone-deep exhaustion that doesn’t improve with sleep.
- Itching (pruritus): 78% deal with this. It’s not just skin deep. Many describe it as if something is crawling under their skin-or worse, inside their bones. It gets worse at night.
- Abdominal discomfort: Dull, persistent pain in the upper right side.
- Jaundice: Yellowing of the skin and eyes when bile backs up.
One Reddit user, u/PSCWarrior, wrote: "The itching is unbearable-it’s not just skin deep but feels like it’s coming from my bones." That’s not exaggeration. It’s real, and it’s disabling.
No Cure. But There Is Care.
Here’s the hard truth: there’s no medication that stops or reverses PSC. Ursodeoxycholic acid (UDCA), once widely prescribed, has been shown in multiple trials to do nothing for survival-and at high doses, it may even increase risk. The European Association for the Study of the Liver now advises against routine UDCA use.
So what’s left? Managing symptoms and preventing complications.
For itching: Doctors may try rifampicin (150-300 mg daily), which works in about half of patients. Naltrexone (50 mg daily) helps when itching is tied to opioid pathways. Colesevelam, a bile acid binder, can reduce bile buildup in the blood.
For vitamin deficiencies: Because bile isn’t flowing properly, fat-soluble vitamins (A, D, E, K) aren’t absorbed. Quarterly blood tests and supplements are critical.
For cancer risk: PSC raises your lifetime risk of colorectal cancer to 10-15% and cholangiocarcinoma (bile duct cancer) to 1.5% per year. That’s why colonoscopies every 1-2 years and annual MRCP scans are non-negotiable.
For infection: If you develop fever, chills, or severe right-side pain, it could be cholangitis-an infection in the bile ducts. That’s a medical emergency.
The Only Real Solution: Liver Transplant
When the liver fails, transplant is the only option. And it works. Over 80% of PSC patients survive at least five years after transplant. Many go on to live full, active lives.
But transplant isn’t a cure. The disease can, rarely, come back in the new liver. And waiting for a donor can take years. That’s why managing progression and delaying liver failure is so important.
What’s on the Horizon?
There’s real hope on the horizon. New drugs are in late-stage trials:
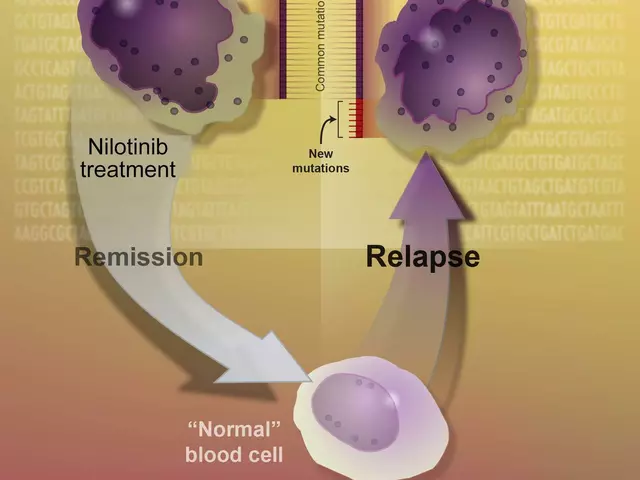
- Cilofexor: A non-steroidal FXR agonist that reduced ALP levels by 41% in phase 2 trials. The European Medicines Agency granted it orphan drug status in early 2023.
- Obeticholic acid: Showed a 32% drop in liver enzymes in phase 3 trials, though safety concerns are delaying FDA approval.
- NorUDCA: A modified bile acid being tested to reduce liver damage without the risks of regular UDCA.
Researchers are also studying how to repair the gut-liver axis-using probiotics, fecal transplants, or targeted antibiotics to reset the microbiome. Early results are promising.
Dr. Andrew Manns of Hannover Medical School predicts: "Within five years, we’ll have at least two disease-modifying therapies." That’s not hype. It’s based on real, ongoing data.
Living With PSC: What Patients Say
On community forums, patients share what really matters:
- "I waited four years for a diagnosis. My doctor thought it was IBS."
- "No one told me about vitamin D. I was bone-deep deficient and didn’t even know."
- "Finding a PSC specialist made all the difference. My fatigue dropped by 60% in six months."
Patients treated at specialized PSC centers report 85% better symptom control than those in general hepatology clinics. Access to these centers isn’t equal-72% of U.S. patients live within 100 miles of one. In rural Europe, that number drops to 35%.
And while funding for PSC research is minimal-just $8.2 million from the NIH in 2022, compared to $142 million for fatty liver disease-patient-led registries like PSC Partners Seeking a Cure are filling the gap. With over 3,100 patients tracked across 12 countries, they’re accelerating discovery.
What You Should Do If You Suspect PSC
If you have chronic fatigue, unexplained itching, or a history of ulcerative colitis, ask for:
- A liver enzyme panel (especially ALP and GGT)
- An MRCP scan
- Referral to a hepatologist who specializes in cholestatic liver diseases
Don’t wait for symptoms to get worse. Early detection means better management. And if you’re already diagnosed: stay in care, get your vitamins checked, know your cancer screening schedule, and connect with others. You’re not alone.
Is Primary Sclerosing Cholangitis the same as Primary Biliary Cholangitis?
No. PSC and PBC are both autoimmune liver diseases, but they’re different. PSC affects both large and small bile ducts inside and outside the liver, and is strongly linked to ulcerative colitis. PBC mainly attacks the small bile ducts inside the liver and is marked by anti-mitochondrial antibodies (AMA) in 95% of cases. PSC has no single antibody marker, while PBC does. They’re treated differently, and their long-term risks vary.
Can PSC be reversed with diet or supplements?
No. There’s no diet, supplement, or herbal remedy proven to reverse PSC. While maintaining good nutrition and taking fat-soluble vitamins (A, D, E, K) is essential to prevent complications, these don’t stop the disease. Avoid unproven treatments-some can even harm your liver. Stick to evidence-based care from a specialist.
Why is liver transplant the only cure?
Because PSC destroys the bile ducts and liver tissue over time. No current drug can repair that scarring or restore bile flow. A transplant replaces the damaged liver with a healthy one, eliminating the source of the problem. While the disease can rarely return in the new liver, transplant restores normal function and dramatically improves survival-80% of patients live at least five years after surgery.
How often should I get tested if I have PSC?
You should have liver enzyme tests every 3-6 months, annual MRCP scans to monitor bile duct changes, and colonoscopies every 1-2 years due to the high risk of colorectal cancer. Vitamin levels (A, D, E, K) should be checked quarterly. If you develop new symptoms like fever, jaundice, or worsening pain, seek care immediately-these could signal cholangitis or cancer.
Is PSC hereditary?
It’s not directly inherited like a single-gene disorder, but genetics play a strong role. If you have a close relative with PSC, your risk is higher. The HLA-B*08:01 gene variant increases risk by over two times. However, most people with this gene never develop PSC-something in the environment triggers the disease. Family history matters, but it’s not destiny.
Can I still work and live normally with PSC?
Many people do-especially with good care. Fatigue and itching can be managed with medication and lifestyle adjustments. Regular exercise, good sleep hygiene, and avoiding alcohol are key. The biggest challenge is emotional: the uncertainty, the waiting, the feeling of being unheard. Connecting with support groups and seeing a specialist who understands PSC can make all the difference in maintaining quality of life.




Robert Bliss
10 March 2026 - 01:56 AM
This post hit me right in the feels. I’ve been living with PSC for 7 years and honestly? Most docs don’t get it. I’m on rifampicin now and it helps with the itching but damn, some nights it still feels like ants are crawling under my skin 😩
Peter Kovac
11 March 2026 - 09:42 AM
The assertion that UDCA is ineffective is supported by multiple randomized controlled trials, including the USPSC trial (2010) and the PRIMIS study (2018). However, the claim that 'no medication stops or reverses PSC' is misleading. While no drug has demonstrated disease-modifying efficacy in phase 3 trials, emerging FXR agonists like cilofexor show statistically significant reductions in ALP (p < 0.001) and are currently under FDA priority review.
APRIL HARRINGTON
12 March 2026 - 07:40 AM
I just found out my dad has PSC and I’m crying because no one talks about this and I feel so alone and also like I’m going to lose him and why is there no cure yet like why is no one funding this like it’s not fair I hate that people think it’s just liver stuff like it’s not just liver stuff it’s everything
Leon Hallal
13 March 2026 - 14:27 PM
I’ve been following this for years. I was misdiagnosed with IBS for 5 years. By the time they figured it out, my ALP was over 1000. I’m on vitamin D, E, K. I take 4 pills a day. I’m 38 and already feel like I’m 70. No one cares. No one talks about the fatigue. It’s not tired. It’s like your bones are made of wet cement.
Judith Manzano
14 March 2026 - 16:32 PM
This was so well written. I’m a nurse and I work with liver patients, but I didn’t know half of this. The gut-liver connection is fascinating. I’ve started sharing this with my patients who have ulcerative colitis. Early MRCP could change lives. Keep spreading awareness - you’re doing amazing work.
rafeq khlo
15 March 2026 - 10:40 AM
The article neglects to mention that PSC is primarily a Western disease caused by overconsumption of processed foods and antibiotics which disrupt the microbiome. In countries with traditional diets, incidence is negligible. Furthermore, the NIH funding disparity is not accidental - it reflects the pharmaceutical industry's disinterest in rare diseases that cannot be monetized through daily pills. Transplant is a profit-driven solution, not a cure
Jazminn Jones
15 March 2026 - 11:00 AM
The reliance on MRCP for diagnosis is outdated. High-resolution elastography and serum bile acid profiling are more sensitive and cost-effective. The article’s emphasis on transplant as the only viable endpoint is clinically naive. Prognostic modeling using AI-driven biomarkers (e.g., miR-122, CK-18) has demonstrated predictive accuracy exceeding 89% in recent cohorts. This is not a conversation for lay audiences.
Scott Easterling
17 March 2026 - 09:22 AM
Wait… so they’re saying there’s NO cure? But what about the guy on YouTube who drank 10 gallons of apple cider vinegar a day and ‘healed’ his liver? And what about that 2019 TikTok trend where people did 3-day liver cleanses? I’m not saying it’s science… but… I mean… what if? Also, why do they keep saying ‘bile ducts’ like it’s a secret code? I think this is all a Big Pharma scam.
Mantooth Lehto
18 March 2026 - 08:15 AM
I’ve been through this. I had cholangitis last year. Fever. Chills. ER. They thought it was gallstones. Took 48 hours to realize it was PSC-related. I screamed at the nurse. I cried in the parking lot. I still do. I’m on naltrexone. It helps. But the loneliness? That’s the real disease. If you’re reading this and you’re alone… I see you. 🖤
Mary Beth Brook
19 March 2026 - 20:25 PM
PSC is not an autoimmune disease. It is a consequence of chronic biliary obstruction secondary to environmental toxins and industrial pollutants. The HLA association is a red herring. The real epidemic is in the Midwest due to glyphosate exposure in groundwater. Transplant is a band-aid. We need systemic policy reform. Not more trials. Not more drugs. Accountability.