
Sulfonamide Cross-Reactivity Checker
This tool helps you understand which medications are safe to take based on your specific reaction history to sulfonamide antibiotics.
Most people who say they have a "sulfa allergy" don’t actually need to avoid all medications with "sulf" in the name. The confusion is widespread, costly, and sometimes dangerous. A 2022 study found that 3 to 12% of people in the U.S. report a sulfa allergy - but only about 0.3% of those people have a true IgE-mediated reaction. The rest are often misdiagnosed. A mild rash that showed up a week after taking sulfamethoxazole-trimethoprim? That’s not a true allergy. It’s a common side effect. Yet, that label sticks - and it changes how doctors treat you for years.
What Exactly Is a Sulfonamide?
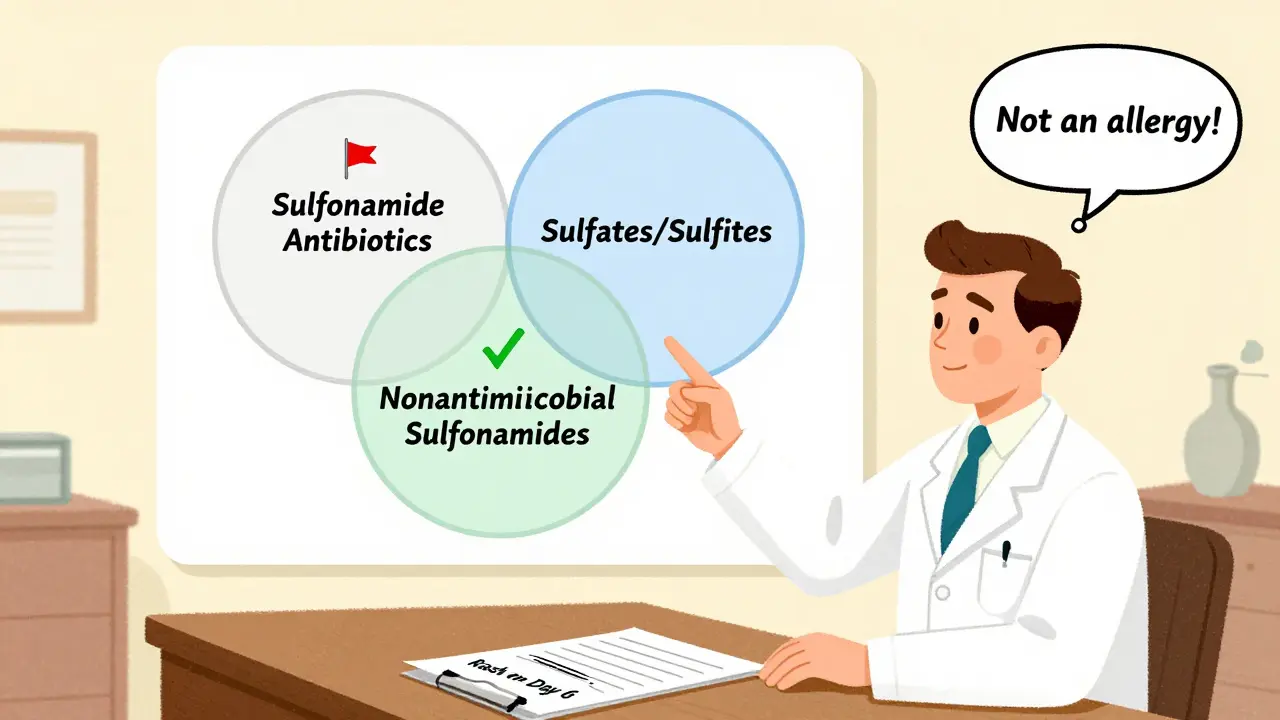
The term "sulfonamide" refers to a chemical group: SO₂NH₂. It shows up in dozens of medications. But not all sulfonamides are the same. The ones that cause real allergic reactions are the sulfonamide antibiotics. These include sulfadiazine, sulfamethoxazole, sulfacetamide, and sulfasalazine. They were the first antibiotics developed in the 1930s and still used today for urinary tract infections, pneumonia, and even some skin conditions.
But here’s the key: these antibiotics have a specific structure - an arylamine group at the N4 position and a nitrogen ring at N1. That’s what makes them allergenic. Other drugs with "sulf" in their name - like hydrochlorothiazide (a blood pressure pill), furosemide (a water pill), celecoxib (Celebrex), and acetazolamide (for glaucoma or altitude sickness) - don’t have that same structure. They’re chemically different. And that difference matters.
Do You Really Need to Avoid Blood Pressure Meds or Arthritis Drugs?
No. Not if your allergy is only to antibiotics.
Multiple large studies confirm this. One study of over 10,000 patients with a documented "sulfa allergy" found that only 1.3% reacted to nonantimicrobial sulfonamides like hydrochlorothiazide. The control group - people without any sulfa allergy label - had a 1.1% reaction rate. That’s not a difference. That’s noise.
Yet, doctors still avoid prescribing these drugs. A 2021 study showed that patients labeled with a sulfa allergy are 2.4 times more likely to get fluoroquinolones like ciprofloxacin or levofloxacin instead of sulfamethoxazole. That’s a problem. Fluoroquinolones carry black box warnings for tendon rupture, nerve damage, and aortic aneurysm. Sulfamethoxazole doesn’t.
Same goes for celecoxib. Many patients with a "sulfa allergy" are told they can’t take it, even though it’s often the best NSAID for arthritis in people with stomach issues. The risk of reaction? Less than 1.5%. That’s lower than the risk of reacting to ibuprofen.
What About Sulfur, Sulfates, or Sulfites?
They’re not the same. And they’re not related.
"Sulfa" is not sulfur. It’s not sulfate (like magnesium sulfate used in preeclampsia). It’s not sulfite (found in wine or dried fruit). These are completely different chemicals. Yet, a 2020 survey found that nearly half of primary care doctors mistakenly think patients with a sulfonamide allergy must avoid all of them. Patients pick up on this. They start refusing medications they don’t need to avoid.
If you’ve ever been told you can’t take a diuretic or a glaucoma eye drop because of a "sulfa allergy," you’ve been misinformed. That’s not science. That’s outdated fear.
Who Actually Has a Real Sulfonamide Allergy?
True sulfonamide antibiotic allergies are rare - but they exist. They usually show up as:
- Immediate reactions within an hour: hives, swelling, trouble breathing
- Severe skin reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis
- Systemic reactions: fever, liver damage, blood cell changes
If you had any of these - especially within hours of taking the drug - you likely have a true allergy. But if you got a mild rash five days after starting sulfamethoxazole? That’s not an allergy. That’s a common, non-allergic reaction. It doesn’t mean you can’t take it again.
And here’s the thing: if you’ve had a severe reaction in the past, you should avoid all sulfonamide antibiotics. But you still don’t need to avoid celecoxib, hydrochlorothiazide, or furosemide. The structure is different. The immune system sees them as different.
Dapsone Is the Exception
There’s one nonantimicrobial sulfonamide that’s different: dapsone.
Used for leprosy, certain rashes, and Pneumocystis pneumonia prevention, dapsone shares structural similarities with sulfonamide antibiotics. Studies show about 13% of people with a true sulfonamide antibiotic allergy react to dapsone. That’s high enough to warrant caution. If you need dapsone and have a history of severe reaction, talk to an allergist. A supervised challenge may be needed.
But for everything else? The risk is negligible.

Why Does This Mislabeling Matter?
It’s not just about convenience. It’s about public health.
When doctors avoid sulfonamide antibiotics because of a mislabeled allergy, they turn to broader-spectrum drugs. That drives antibiotic resistance. A 2021 study found that patients with a "sulfa allergy" label were 78% more likely to get an alternative antibiotic - and 33% of those alternatives were unnecessarily broad. That means more resistant E. coli, more resistant staph, more hard-to-treat infections.
The cost? Over $1.2 billion a year in the U.S. alone. Extra hospital stays. Longer treatments. More side effects.
And for patients? It means being stuck on less effective, more toxic drugs for years. One man in his 60s avoided hydrochlorothiazide for 15 years because of a childhood rash. He ended up with uncontrolled blood pressure. Only after an allergist did a simple oral challenge did he get the right medicine - and his blood pressure dropped to normal within weeks.
What Should You Do?
If you’ve been told you have a "sulfa allergy," ask yourself: What exactly happened? When? How soon after taking the drug?
Here’s what to do next:
- Check your medical records. Does it say "sulfa allergy" - or does it say "mild rash on day 6 of sulfamethoxazole"?
- If it’s vague, ask your doctor if you can be evaluated. Many clinics now offer sulfonamide allergy de-labeling programs.
- If your reaction was mild and delayed, you may be able to safely take nonantimicrobial sulfonamides - and even sulfonamide antibiotics again - under supervision.
- If your reaction was severe (anaphylaxis, skin blistering), avoid all sulfonamide antibiotics. But still, nonantimicrobial sulfonamides are likely safe.
Don’t let a label from 20 years ago limit your treatment options today. Science has moved on. Your care should too.
What About the Future?
There’s new hope. In 2022, researchers developed the SULF-RISK score - a tool that uses your reaction history to predict if your allergy is real. It’s 92% accurate. And by 2025, most major hospitals will have automated alerts in their electronic systems that flag vague "sulfa allergy" labels and suggest de-labeling.
There’s also a blood test in development - one that looks for IgE antibodies specific to sulfamethoxazole. Early results show it’s 90% accurate. That means one day, instead of guessing, doctors will know for sure.
For now, the best tool you have is knowledge. Don’t assume. Ask. Clarify. Challenge the label if it doesn’t fit your history.
Can I take hydrochlorothiazide if I have a sulfa allergy?
Yes, you can. Hydrochlorothiazide is a nonantimicrobial sulfonamide. It doesn’t have the same chemical structure as sulfonamide antibiotics like sulfamethoxazole. Studies show the risk of reaction is no higher than in people without any sulfa allergy label. Most patients with a history of mild rash from antibiotics tolerate hydrochlorothiazide without issue.
Is celecoxib (Celebrex) safe for people with sulfa allergy?
Yes. Celecoxib is a nonantimicrobial sulfonamide. It lacks the arylamine group that triggers allergic reactions in sulfonamide antibiotics. Multiple large studies show reaction rates are similar to the general population. Avoiding it unnecessarily means missing out on a safer NSAID option for many people, especially those with stomach sensitivity.
What’s the difference between sulfonamide, sulfate, and sulfite?
They’re completely different. Sulfonamides are a class of drugs with a specific chemical group (SO₂NH₂) that includes antibiotics like sulfamethoxazole. Sulfates (like magnesium sulfate) are salts used in medicine for seizures or constipation. Sulfites are preservatives in wine and dried fruit. None of these trigger the same immune response as sulfonamide antibiotics. If you’re allergic to sulfonamide antibiotics, you don’t need to avoid sulfates or sulfites.
Can I take sulfonamide antibiotics again after having a rash?
If your rash was mild and appeared more than 72 hours after taking the drug, you likely didn’t have a true allergy. Many people who had this type of reaction can safely take sulfonamide antibiotics again - especially under medical supervision. A simple oral challenge, done in a clinic, can confirm tolerance. This is now a standard practice in allergy clinics.
Why do doctors still avoid prescribing sulfonamides if the risk is low?
Because outdated labels persist in medical records. Many doctors aren’t trained in allergy interpretation. They see "sulfa allergy" and assume it means "all drugs with sulf in the name." Electronic health records are starting to fix this, but change is slow. If you’ve been mislabeled, you may need to advocate for yourself - or see an allergist to get your record corrected.
Is dapsone safe if I have a sulfa allergy?
It’s not always safe. Dapsone shares structural similarities with sulfonamide antibiotics and has a higher cross-reactivity risk - about 13%. If you’ve had a severe reaction to a sulfonamide antibiotic, you should avoid dapsone unless tested by an allergist. A supervised challenge can determine if you can tolerate it.





Radhika M
17 December 2025 - 12:59 PM
So if I had a rash from Bactrim years ago, I can still take hydrochlorothiazide? That’s a game-changer. My doc kept giving me expensive alternatives and I never asked why. Thanks for clearing this up.
Martin Spedding
18 December 2025 - 04:20 AM
lol so now we’re supposed to trust meds with ‘sulf’ in the name again? sure. next they’ll say penicillin’s fine if you’re ‘not *really* allergic’
Josh Potter
18 December 2025 - 14:10 PM
YOOOO this is wild. I’ve been avoiding ALL sulfa stuff since I got a rash at 14. Turns out I could’ve been on blood pressure meds that actually WORKED? My BP’s been a nightmare for 12 years bc of a stupid label. This needs to be on every doctor’s wall.
Evelyn Vélez Mejía
19 December 2025 - 05:02 AM
The persistence of this misinformation represents a profound failure of medical education and institutional inertia. The conflation of chemical classes is not merely an oversight-it is a systemic epistemological error that compromises patient autonomy and public health. We must interrogate the ontological foundations of diagnostic labeling in pharmacology.
Victoria Rogers
19 December 2025 - 20:57 PM
USA still letting people die from bad science. Other countries know this. Why are we still behind? Also celecoxib is just Big Pharma’s way to make you pay more. Trust nothing.
Jane Wei
20 December 2025 - 09:51 AM
my grandma got mislabeled with a sulfa allergy in the 80s. she’s been on weird meds ever since. this is the kind of thing that should be in every medical school lecture.
Jody Patrick
21 December 2025 - 13:21 PM
So dapsone’s the only one? Got it. That’s it. No more drama.
Philippa Skiadopoulou
21 December 2025 - 18:32 PM
Highly informative. The distinction between antimicrobial and nonantimicrobial sulfonamides is clinically significant and underappreciated. Documentation of reaction timing is essential for accurate de-labeling.
Pawan Chaudhary
21 December 2025 - 20:37 PM
This is so helpful! I’ve been scared to take any med with ‘sulf’ since I was a kid. Now I feel like I can finally ask my doctor without feeling dumb 😊
CAROL MUTISO
22 December 2025 - 17:46 PM
Oh so you mean all those years I avoided diuretics because I got a rash from antibiotics… was just my body being extra dramatic? And now I’m paying $200 a month for a pill that’s basically the same thing? Brilliant. Thanks for the 2024 version of ‘your mom was wrong.’
Virginia Seitz
24 December 2025 - 03:25 AM
YASSS this is why I love science 🙌 I told my doc last year I didn’t think I was allergic, and they just shrugged. Now I’m gonna bring this article. Time to fix my records!
amanda s
24 December 2025 - 19:42 PM
So you’re saying the government let 12 million people suffer because doctors are lazy? And now you want us to trust them again? NOPE. I’m not risking it. My rash was BAD.
Peter Ronai
26 December 2025 - 07:28 AM
Wow. Another ‘science says’ article from someone who doesn’t understand immunology. Allergic reactions are complex. You can’t reduce them to ‘chemical structure.’ You’re putting lives at risk with this oversimplification.
Steven Lavoie
26 December 2025 - 12:34 PM
Thank you for writing this with such clarity. I’ve seen patients avoid life-saving medications for decades because of a single misdiagnosed rash. This isn’t just about drugs-it’s about dignity. People deserve accurate information, not fear-based protocols.
Michael Whitaker
28 December 2025 - 10:27 AM
As a former clinical pharmacologist at Johns Hopkins, I must emphasize: while the structural argument holds theoretical merit, the clinical literature on cross-reactivity remains inconsistent. To generalize this as ‘safe’ for all nonantimicrobial sulfonamides is a dangerous oversimplification that ignores individual immune variability and potential epigenetic factors.